How can the implementation of an innovative management system impact on the activities of a simulation centre? What kind of data can the use of such an advanced system provide? We find the answers in this case study carried out by Medcam in a Polish university.
Content written in collaboration with Medcam.
The case study was developed based on the implementation of the Medcam PRO system at one of the medical simulation centres in Poland in August 2022. The analysis was made on the basis of data collected in the Medcam PRO system during the winter and summer semesters of the 2022/2023 academic year and made available by this University to the Medcam brand after we received the appropriate approval. The data presented has been anonymized, and the trade names of the equipment at the unit’s disposal have been removed.

Introduction
Each SIM centre is at a different point in its growth and has distinct needs. These differences are determined by the geographic region, experience, the unit’s budget, the standard of education, the work culture and other factors, such as the number of majors, students, subjects, courses taught, the number of simulation labs and equipment owned. Not to forget the number of staff, the duties of employees, the goals of the unit, the level of computerization implemented, and many others not mentioned here. All these factors form the specifics of each Simulation Center and require individual planning.
Precontemplation stage, or awareness of needs
The element that unites various centres is the specificity of medical simulation, where both educational and training goals are very similar. However, the way each facility manages and operates can be quite different.
Very often, units that have not implemented professional solutions intended for them, rely on the exchange of information between educators (instructors), technicians, SIM centre management and administrative staff through, for example, e-mails or phone calls. However, the unreliability of such solutions is very high. Therefore, the need to improve the information flow process was the most important argument for making changes in the organisation of the SIM centre work of the case in review.
Step one – preparing for the implementation of the management system
The first step was to establish the new SIM centre operating rules and the necessary paperwork, i.e. to modify the SIM centre’s working regulations based on the system’s available functionalities. The Medcam PRO system gave the possibility to customise the configuration of the department according to the individual needs of the end users, like for example, the number of employees or the opening hours of the facility. The next step was to add to the system simulation rooms, warehouses and subjects taught at the Center, as well as owned equipment.
This process was carried out using the file import mechanism provided by Medcam PRO, which greatly reduced the time needed to create the foundation of the implementation – the database about the department. After that, it was completed with additional information about the equipment, i.e. upcoming inspection dates, manufacturer’s specifications – both in the form of descriptions, photos and external links.
Step two – trainings
The next step was to add users to the system and conduct training on how to use it. Training was a key part, because it also included the creation of scenarios and assessment cards that users will use in the future. Therefore, the training involved not only technicians, but also academics and management. The implementation of the system was carried out before the new teaching semester began, thus at the best time for it, as it allowed the SIM centre to collect data on its work throughout the full academic semester. When planning the implementation, it was also necessary to take into account the transition period necessary for the reprocessing of the various steps, which, with regard to the case described, was 2 weeks.

Step three – complete system implementation
All communication and information exchange at the SIM centre has so far been done in person, through e- mails and by phone calls. Since the implementation of the management system, communication has moved exclusively to the Medcam PRO system. Upon joining the system, the work of users has changed as follows:
Teachers – the scenarios and assessment cards added to the system are used by them in their demands for classes when they book simulation rooms and necessary equipment for exams and simulation sessions. Users can share scenarios and assessment cards with other teachers in the department, nationally and internationally, which has enabled closer inter-teacher and cross-university cooperation. Remote access to equipment and equipment placement in the SIM centre has translated into better and more thoughtful use of resources when making requests for classes, or for additional courses.
Technicians – on the basis of demands made, a schedule of classes is created automatically – including rooms and equipment booking, with the possibility of editing, accepting/rejecting and changing classes statuses by technical staff, which has greatly facilitated the flow of information within the team. Specific technicians or specific standardised patients can be assigned to classes, and also exams can be scheduled. So that, the team of technicians now has clearly assigned tasks and each technician can check in the system the stage of preparation for a particular class. The schedule of classes can be displayed in the hallways where students congregate and on the SIM centre website, so any interested person has now access to up-to-date information about scheduled classes without needing to ask any staff.
Executives – they have gained full control over the current work of the centre, including: information on simulation rooms occupancy, equipment usage, consumption of disposable materials, scenarios and assessment cards, as well as demand for standardised patients. All data entered into the system can be exported to Excel or pdf files, which provides great opportunities to analyse the work of the SIM centre and to plan the demand for disposable materials for each major, for the services of standardised patients, and also allows to estimate the possibility of conducting additional classes using medical simulation. The system also allows to generate reports based on selected date ranges and selected values that we want to analyse, so filtering the relevant data and developing reports on the unit’s activities has become much easier and more precise, and most importantly, the collection of this data did not require administrative staff to do additional work and maintain separate data sets.
Information about the department and the scale of implementation of the system
- Majors: Medicine, English Division, Nursing (1st and 2nd degree), Midwifery (1st and 2nd degree), Emergency Medicine.
- Other Activities (Other): External and internal trainings, courses, conferences, workshops
- Number of users in the system: 106 people (excluding students)
- Classrooms in the system – total: 54
- Subjects, including additional initiatives at SIM centre – total: 84 (incl. trainings, courses)
- Equipment: simulators/phantoms/trainers – total: 475 items
- Equipment: medical equipment – total: 1,160 items
- Equipment: disposable materials – total: 548 different items
- Scenarios – total: 201
- Assessment cards – total: 160
- Requests made – total: 1762

The main advantages from the implementation of the system:
- Online access to the system for all employees 24/7/365 days
- Access to complete information in one place, displayed according to the user’s privileges, enabling effective information management
- Rapid onboarding of new employees
- Standardised form and scope of the information provided necessary to conduct classes
- Common database of scenarios and assessment cards in the system
- In case of sudden absence of an employee, information about the status of preparation and scheduling of classes available to the rest of the staff at glance, without disturbing the rest of the absent employee, and if necessary, the completion or correction of urgent information by him/her in the system – also possible from home
- Possibility of partial remote work
- Clear-cut and more precise definition of needs and requirements for the preparation of classes
- More efficient work in the preparation and implementation of classes
- Full control over equipment and disposable materials
- Purchase requests for disposable materials and equipment made with greater precision and corresponding to real needs, even if the demand is made by an employee without many years of professional experience,
- Automatic reminders for equipment inspections
- Ability to generate statements and reports
The biggest challenges and difficulties encountered during system implementation:
- Reprocessing changes to the existing SIM centre operation regulations
- Training of employees at one time
- Upholding the new standards
- Resistance from employees due to fear of change (marauders)
The results of selected data generated from the Medcam PRO system in the winter and summer semesters of 2022/2023 can be downloaded here.
Notes
This case study covers the analysis of only a small part of the data collected in the Medcam PRO system.
The data collected were analysed taking into account full clock hours, not teaching hours (data presented according to ggg:mm:ss format). The analysis of equipment used was presented without indicating information on manufacturers, equipment models and the exact number of hours of use of each piece of equipment.
The total time spent using simulators and medical equipment included all available devices of the same type.The same data presentation method was used for disposable materials – the amount of used materials of one type was summed, e.g. needles of different sizes, but it is possible to analyze individual items. Local administrators using the Medcam PRO system can analyse the data based on their own assumptions and create their own summaries, such as the occupancy of rooms in relation to days of weeks/hours/weekends, the number of working hours of use of each piece of equipment, and a list of equipment that is least used or not used at all during the course of classes. Only classes with the status “Classes completed by a technician” were analyzed. Classes that were not held were made up at another time as new demands. “Requires improvement” status refers to demands rejected by technicians, in which teachers did not make corrections, but created a new requirement.
Based on the collected results, SIM centre management will be able to better plan the work of employees, better allocate equipment for the implementation of classes to equalise the level of use of this equipment and equalise its lifespan, prepare for the ordering of appropriate single-use materials in the necessary quantities, and present the cost intensity of individual courses, subjects, or additional courses. In addition, the collected data provides an opportunity to calculate the cost of conducting a training course, or a course implemented at the SIM centre, based on the equipment used and the resources involved.
Analysis of results
In the winter semester 2022/2023, classes were held at the SIM center a total of 785 times, while in the summer semester they were held 801 times. The total number of class requests, which corresponds to the number of classes held at the SIM centre, is similar in both semesters, although in the winter semester the number of classes not held is higher. As can be seen from Table 3 and 4, the data differ in the number of majors, as in the summer semester for the master degree programme classes were not held at the SIM centre.
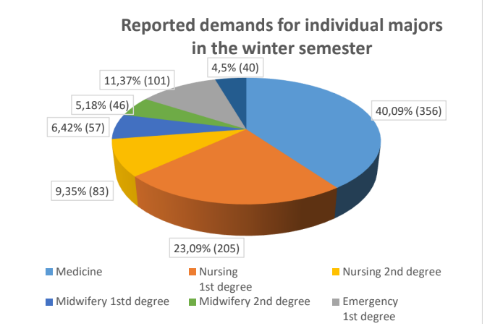
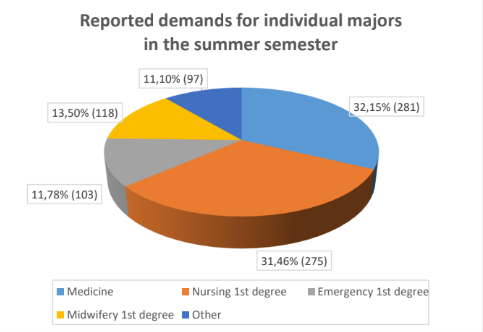
The number of classes and their frequency in each major varies significantly. The largest number of classes took place in the Medicine major and in Nursing, Bachelor degree, the smallest in Emergency Medicine. The graph ‘Other’ refers to the other classes held at the SIM centre, such as external courses and internal training.
The subjects of Medicine major on which SIM centre resources were most frequently used were Emergency Medicine and Medical first aid with elements of nursing. Interestingly, the number of hours completed in Emergency Medicine differed significantly from the number of hours in the other subjects – it was almost three times greater in both semesters than in Anaesthesiology (569h 12min. for Emergency Medicine and 207h 1min. for Anaesthesiology) and about half greater than in Medical first aid with elements of nursing (273h 31min.). The total hours realised in Nursing, Bachelor degree, in the summer semester was almost twice as high as in the winter semester. More than half the shorter duration time of classes realised in the winter semester in Nursing, Master degree, than in Nursing Bachelor degree was evident.
In the Nursing, Bachelor degree classes, the use of medical simulation occurred most frequently in Basics of Nursing (a total of 920h 23min.) and Basics of Emergency Medicine (225h 45min.), while in Master degree of Nursing it occurred in the subject Therapeutic care and education in chronic diseases (94h 15min.). Therefore, from the point of view of the importance of having highly qualified instructors in the most frequently taught subjects, it seems reasonable that the personnel conducting the above-mentioned courses should have the best possible content preparation for teaching using the simulation method. Moreover, it seems equally important to analyse which of the taught subjects should increase the number of practical classes held at the SIM centre in order to improve the level of practical skills acquired by the students of a given course.
Out of 1,762 class requests made throughout the academic year, classes were held a total of 1,586 times, of which 118 times classes were delivered with a standardised patient (SP). Of the 55 classes in 2nd semester involving the SP, 41 of them were OSCE examinations. The total class time involving a standardised patient (an actor) was just over 198 clock hours in the winter semester and almost 356.5 clock hours in the summer semester, of which the examinations involving the SP totalled 293h and 6min. Converting this into teaching hours, for 45minutes each, this results in a demand for 390 hours and 36min of actor work during the 41 OSCE examinations that were conducted in the unit under study during the period under review. Based on these figures, it can be assumed that for 100% of the planned classes at the SIM centre in question, about 6.9-7.6% of them will need the support of SP role-players.
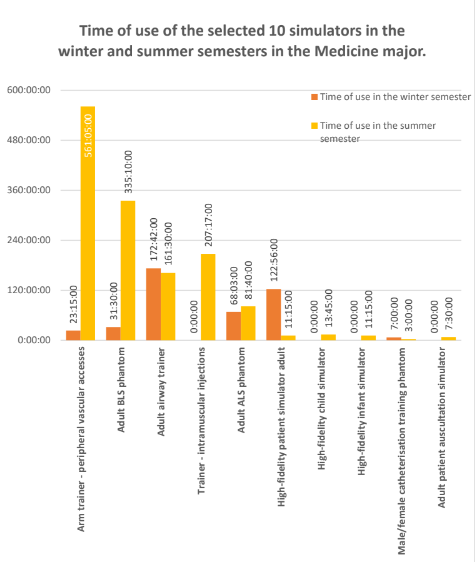
The data exported from the Medcam PRO system provides a very wide range of possibilities for analysing source data on used and unused equipment, thus allowing data to be analysed, for example, in terms of occupancy and the amount of use of specific equipment and the validity of purchase requests, but it is impossible to discuss them in full here. Therefore, this case study only considers a selection of the most common simulators and medical equipment and disposables and compares them with each other in relation to the time of use in different majors.
An arm trainer for peripheral vascular access, an adult BLS phantom, an intramuscular injection trainer and an adult airway trainer were the most used pieces of equipment among those selected for the Medicine major. The adult patient auscultation simulator was used the least – the equipment was used for just 7.5h throughout the year.
The Nursing major used the peripheral vascular access arm trainer, the adult BLS phantom and the adult airway protection trainer most frequently. The high-fidelity child simulators and adult patient simulators were used at Nursing during the study period at a very low level. This leads to the conclusion that it would be advisable to analyse the syllabuses, demands and simulation scenarios on this course and, if the study programme provides for the acquisition of competences, knowledge or skills towards which the use of the phantoms in question could enhance the quality of the classes – motivate the team to use them actively or organise training sessions reminding them of the possibilities of their application in practice, in order to fully exploit the potential of the SIM centre resources and enhance the quality of the classes.
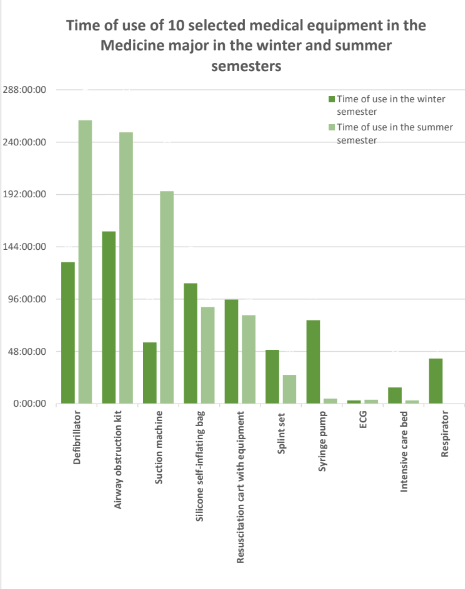
Of the medical devices analysed, the most frequently used in Medicine major in the analysed period were an airway management set (407h 9min.), a defibrillator (390 hours) as shown in Table 20-22, and in nursing – a silicone self-inflating bag (as many as 518h 15min.) and a syringe pump (520h 15min.), which seems to be in line with the skills that students of these majors should have. Of the equipment selected for this analysis, the ECG showed the least use during the Medicine classes, with only 6h and 45min of use, while the respirator was not used at all on Nursing, Bachelor degree major. It was, however, used in the winter semester on the Nursing, Master degree major for 131h 15m.
An analysis of the use of disposable materials showed the highest use of almost the same disposable materials. Nursing used a total of significantly more needles – 2769 pieces compared to the medical faculty, where needle consumption was almost three times lower – 950 pieces. The nursing faculty also used 1023 pieces of intravenous cannulas, 1905 syringes and 1207 pieces of sterile gauze. In the Medicine major, the consumption of these disposables was 943, 585 and 69 pieces respectively. The usage of the smallest number among the selected ‘disposable’ items for the Medicine major was for upper airway suction catheters (1 item) and Foley catheters (2 items) and NaCl 0.9% drips (3 items). For Nursing majors, these were Foley catheter (8 items), elastic and tourniquet (14 items) and NaCl 0.9% drip (15 items). From the above data, it can be seen that after analysing the number of students and prices of items respectively, as well as the amount of disposable materials that each major consumed, it will be possible to determine the average cost of living per student and which major requires the greatest financial outlay, which will be important information for budget planning for each faculty.
The Medcam PRO system also provides the opportunity to analyse the work of the technicians working at the SIM centre. This case study examines how often a technician is assigned to the preparation and delivery of classes. It is also possible to analyse this data in relation e.g. to the subjects to which the technician is assigned most often, what percentage of requests was completed by the technician in question and what percentage of demands was rejected, etc. From the data analysed, it can be seen that among the technicians assigned consecutive numbers, technician 4. handled the most classes in 2nd semester (202 demands with a total duration of 947h and 24 minutes, representing 25.11 % of all demands in 2nd semester). Technicians 8. and 9. were responsible for 13.48% and 15.36% of the classes served, respectively. The other technicians organised for less than 10% of the classes each. This disparity may be due to a number of factors. With regard to the case in question, it was mostly due to staff changes that took place during the semester under analysis and the division of tasks between technicians in force at the SIM centre in question. Therefore, when analysing any data before making binding decisions affecting the entire organisation, it is worth considering additional factors and seeking comment from those who may have complementary data.

Summary
According to the innovation diffusion curve, known as the Roger’s model (Everett M. Rogers, 1982), innovators who like to take risks and try new things represent only 2.5% of the population, early adopters 13.6% – they are leaders, shape opinion in the community, but buy novelties with some caution. The early majority, assimilating the new product earlier than the average buyers represent 34% of the population. The late majority, 34%, are the sceptics who accept the product after others have tried it. The last group are the marauders – 16%, a group of buyers who fear change and absorb an innovation when it becomes common or necessary. When implementing new solutions in an organisation, it is important to take into account that staff, like the management division, will manifest the behaviours of each of these groups, and managers and those responsible for implementing changes at the SIM centre will have to deal with all staff reactions. Therefore, the implementation of an innovation can have positive or negative effects, depending on whether the process is managed correctly. In the case in question, the effects have been positive and, in the long term, it has brought order to the work of the department and helped to notice some facts. However, it should be noted that the SIM centre management system becomes of real value once the data is entered and the entire team starts working on it. Only when this is achieved can the flow of information and the quality of work at the SIM centre be improved.
READ ALSO